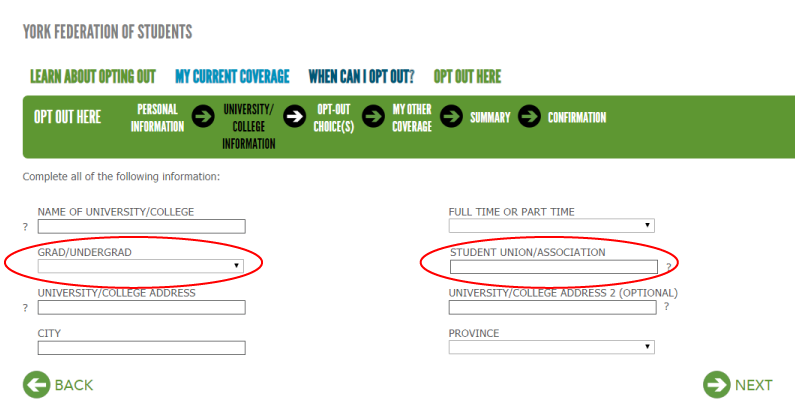
step by step guide
How To Opt Out
All Opt-out Applications for Fall and Winter students are now closed.
Fall 2024 deadline: October 18, 2024
Winter 2025 deadline: February 7, 2025
The Fall Term opt-out application is only available for students beginning their studies in the Fall 2024 term. The deadline to fill this out was October 18, 2024.
The Winter Term opt-out application is only available for students beginning their studies in the Winter 2025 term. The deadline to fill this out was February 7, 2025. Students who began in the Fall 2024 term are not eligible to opt out of the plan during the Winter 2025 opt-out window.
Please be sure to read this page for all steps on how to opt-out.
Please note if your opt-out application is successful, it takes up to three weeks for the refund.